Solving Complex Cranial Defects: Bilateral Craniotomy and Frontal Bone Reconstruction
Not all cranioplasty cases present equal levels of technical demand. A unilateral parietal defect with well-defined margins and minimal prior surgical history is a fundamentally different reconstruction problem from a large bilateral frontal defect in a patient with multiple prior operations, retained hardware, and compromised soft tissue coverage. The latter category (encompassing bilateral craniotomies, extensive frontal bone defects, and cases with complicating factors such as retained mesh or bone fragments) represents the high end of complexity in cranial reconstruction.
This article addresses the specific challenges presented by complex cranial defect cases and the design and manufacturing approaches that best serve them.
Defining Complex Cranial Defect Cases
Complexity in cranioplasty can be characterized along several dimensions. Defect size is the most obvious: large defects spanning more than one anatomical region require implants with correspondingly larger surface areas and more demanding edge-fit geometry. But size alone does not capture the full picture.
Bilateral craniotomy defects (those crossing the midline) introduce the additional challenge of symmetry. Because the human cranium is bilaterally symmetric under normal conditions, an implant spanning the midline must restore that symmetry in a visible, externally palpable region. Asymmetries that might be acceptable in a posterior defect become conspicuous in the frontal region, where the implant’s contour is reflected in the patient’s forehead profile.
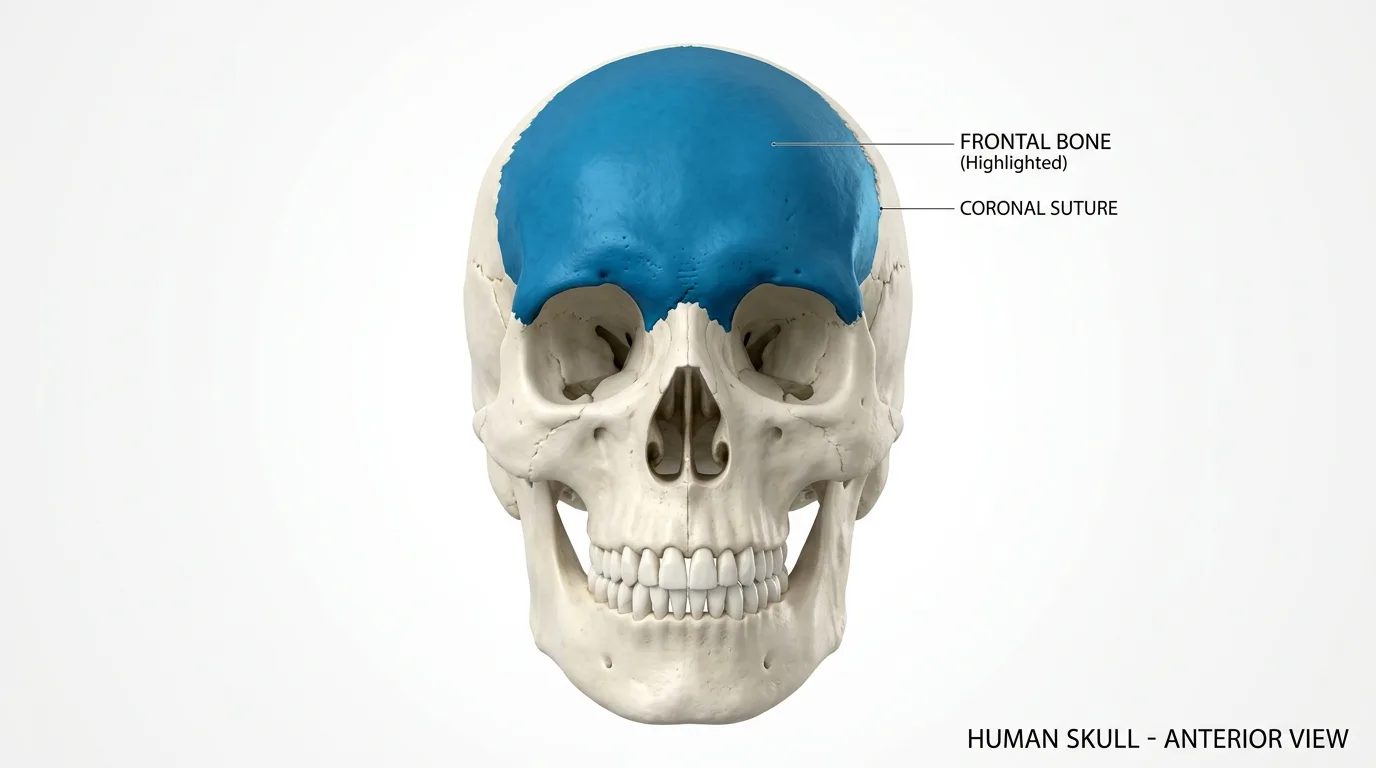
Frontal bone defects carry their own anatomical demands. The frontal bone forms the superior orbital rims, the glabellar region, and the anterior cranial floor. Reconstruction in this area requires attention to how the implant interacts with orbital anatomy, the frontal sinus (when present), and the overlying soft tissue drape. An implant that is geometrically correct in its superior surface but poorly designed at its inferior margins may fail to restore natural facial framing or may create sinus-related complications.
Prior surgical history adds another layer. Patients who have undergone decompressive craniectomy following traumatic brain injury or stroke, or who have had prior cranioplasty attempts, often present with local tissue changes, retained hardware, or modified bone margins that alter the defect geometry from what standard anatomical references would predict.
Decompressive Craniectomy and Secondary Reconstruction
A significant driver of complex cranioplasty volume is the decompressive craniectomy, a procedure performed in acute neurosurgical emergencies to relieve intracranial pressure by removing a large portion of the skull. While the life-saving utility of this procedure is well established, it creates a substantial secondary reconstruction burden.
Decompressive craniectomy defects are often large, involving the frontal, temporal, and parietal regions on one or both sides. The removed bone flap may be preserved for reimplantation, but autologous bone reimplantation carries risks of resorption, infection, and fragmentation that lead many surgical teams to favor alloplastic reconstruction. When alloplastic implants are selected, the implant must be designed to match the contour of a defect that was defined by the emergency craniectomy, which may not have been planned with secondary reconstruction geometry in mind.
Bilateral decompressive craniectomies, while less common, represent the most demanding reconstruction scenario in this category. The implant must restore bilateral cranial contour, manage midline geometry, and integrate cleanly with whatever bone and prior hardware remains.
Implant Design Considerations for High-Complexity Cases
For complex defect cases, the design of the implant (not just its material) has direct implications for surgical outcome. Several design factors merit attention.
Margin geometry determines how the implant interfaces with surrounding bone. A well-designed implant has margins that conform closely to the defect edges, minimizing gaps that could allow implant rocking, fluid accumulation, or fibrous tissue interposition. In cases where bone margins are irregular or beveled, the implant geometry must account for actual defect topography rather than an idealized or simplified representation of it.
Retention and fixation planning should be integrated into the implant design from the outset. Most cranioplasty implants are secured with titanium fixation systems, specifically plates and screws at the implant margins. Designing the implant with appropriate thickness and material properties at fixation zones, and anticipating the location of fixation points relative to defect geometry, supports reliable intraoperative seating.
For cases involving frontal sinus anatomy, the implant design must address whether the sinus will be obliterated or preserved, and the inferior implant geometry must be shaped accordingly. An implant that incompletely covers the sinus opening or creates dead space at the sinus interface introduces risk of mucocele formation or infectious complication.
The Role of Preoperative Modeling
Physical or 3D-printed skull models derived from CT data serve several functions in planning complex cranioplasty cases. They provide the surgical team with a three-dimensional representation of the defect and its surrounding anatomy that is more immediately interpretable than axial imaging slices. They allow for trial fitting and orientation confirmation before the actual procedure.
For bilateral or frontal cases where symmetry is critical, models allow the surgical team to evaluate the projected aesthetic result of the implant before fabrication is finalized. Identifying concerns at the model review stage, rather than at the operative field, is materially more efficient and supports better outcomes.
Models are also useful for trainee education and preoperative briefing of operating room staff, ensuring that the entire team understands the planned reconstruction before the case begins.
Criteria for Selecting a Patient-Specific Implant Manufacturer
Surgeons managing complex cranioplasty cases face a practical choice in selecting a manufacturing partner. For routine cases, many implant fabricators can deliver adequate results. For high-complexity cases, the selection criteria should be more specific.
Relevant factors include the manufacturer’s experience with bilateral and frontal defect geometries, the design review process they apply to complex cases, the level of anatomical expertise involved in implant geometry refinement, and the communication workflow that supports case-specific questions and design iterations before fabrication is committed.
Turnaround time matters in elective reconstruction planning, but it should not be the primary selection criterion for cases where fit quality will have significant operative implications. A well-fitting implant that takes an additional week to fabricate is generally preferable to a poorly fitting implant delivered faster.
Summary
Bilateral craniotomy and frontal bone defects occupy the high end of the cranioplasty complexity spectrum. Managing these cases well depends on accurate imaging, careful implant design with attention to symmetry and regional anatomy, and a fabrication process capable of delivering the geometric precision these cases require. Patient-specific implants, designed from the individual patient’s CT data and refined with appropriate expertise, represent the current standard of care for this population.
For additional context on the design and fabrication pipeline supporting these cases, see the related articles on CT-to-implant workflows and the contribution of medical artistry to implant design.